Manage Diarrhea in Patients Receiving Nerlynx® (Neratinib) Tablets
Nerlynx® (neratinib) tablets, an oral kinase inhibitor, is approved by the U.S. Food and Drug Administration for the extended adjuvant treatment of adult patients with early-stage human epidermal growth factor receptor 2-positive (HER2+) breast cancer, following adjuvant trastuzumab-based therapy.
The recommended dose of neratinib (https://nerlynx.com/pdf/full-prescribing-information.pdf) is 240 mg, taken orally as a single dose of six 40 mg tablets, continuously for one year.
In clinical trials (https://nerlynx.com/pdf/full-prescribing-information.pdf), the most common adverse reactions (ARs) associated with neratinib (occurring in at least 5% of patients) were diarrhea, nausea, abdominal pain, fatigue, vomiting, rash, stomatitis, decreased appetite, muscle spasms, dyspepsia, aspartate/alanine aminotransferase increase, nail disorder, dry skin, abdominal distention, epistaxis, weight decrease, and urinary tract infection.
Severe diarrhea and sequelae, such as dehydration, hypotension, and renal failure, have been reported during treatment with neratinib. The mechanism of action of diarrhea is not known, but the AR is hypothesized to be caused by epidermal growth factor receptor inhibition. Preclinical models suggest that the etiology of neratinib-related diarrhea is multifactorial (https://nerlynx.com/pdf/full-prescribing-information.pdf), including elements of secretory and inflammatory diarrhea and bile acid malabsorption.
As a result, antidiarrheal prophylaxis with loperamide should be initiated with the first dose of neratinib and continued during the first two treatment cycles (56 days) and as needed thereafter, titrated to one to two bowel movements per day; see Table 1 for dosing schedule.
Additional antidiarrheal agents may be necessary for patients with diarrhea. Neratinib dose interruptions and reductions may also be required to manage diarrhea (https://nerlynx.com/pdf/full-prescribing-information.pdf). If diarrhea persists, dose modifications, interruptions, or discontinuation may be indicated. Visit the medication website (https://nerlynx.com/hcp/get-patients-started/dosing-modifications) for a guide to neratinib dose adjustments.
TABLE 1. RECOMMENDED LOPERAMIDE PROPHYLAXIS WITH NERATINIB
|
Time on Neratinib |
Dose |
Frequency |
|
Weeks 1-2 (days 1–14) |
4 mg |
Three times daily |
|
Weeks 3-8 (days 15–56) |
4mg |
Twice daily |
|
Weeks 9-52 (days 57–365) |
4mg |
As needed (not to exceed 16 mg per day) |
Diarrhea Rates in the ExteNET Trial
The phase III ExteNET trial compared outcomes of treatment with neratinib versus placebo in 2,840 women (median age = 52 years) with HER2+ early-stage breast cancer who had completed adjuvant treatment with trastuzumab-based therapy in the past two years. Patients were randomized to receive neratinib (n = 1,420) or placebo (n = 1,420) for one year. Antidiarrheal prophylaxis was not protocol mandated (https://nerlynx.com/pdf/full-prescribing-information.pdf).
Diarrhea occurred in 95% of patients treated with neratinib, with 40% experiencing grade 3 diarrhea and 0.1% experiencing grade 4 diarrhea. The majority of patients (93%) had diarrhea in the first month of treatment, with a median time to first onset of grade 3 or higher diarrhea of 8 days (range = 1–350 days). Treatment-related diarrhea was also short in duration (https://nerlynx.com/pdf/full-prescribing-information.pdf), with a median cumulative duration of grade 3 or higher diarrhea of 5 days (range = 1–139 days).
Findings From the Phase II CONTROL Study
A safety study on the effects of adding budesonide or colestipol to loperamide for neratinib-associated diarrhea
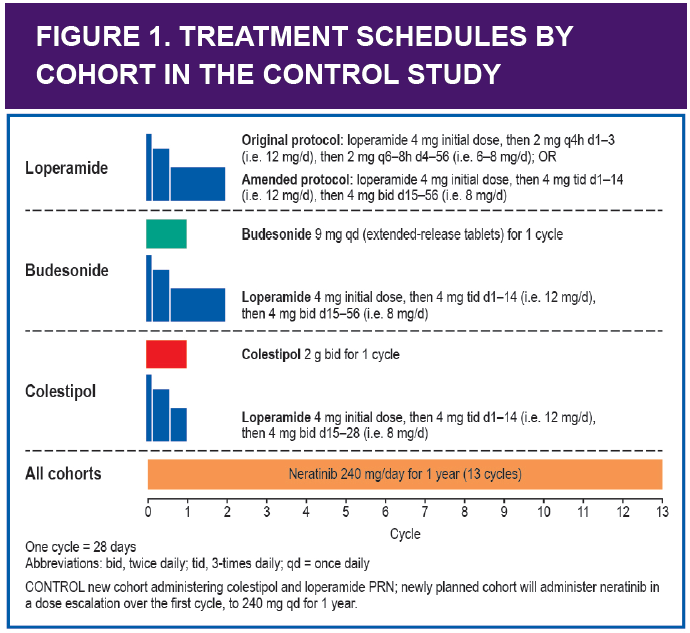
The ongoing, international, sequential-cohort, open-label, phase II CONTROL study is assessing the effects of diarrhea prophylaxis when used in combination with neratinib. The study includes 321 patients with stage 1–3C HER2+ breast cancer who had received trastuzumabbased adjuvant therapy in the past year. All patients received neratinib 240 mg per day for one year, plus loperamide for one to two cycles, followed by loperamide 16 mg per day or less as needed thereafter. Another cohort received add-on budesonide, a locally acting corticosteroid used for inflammatory gastrointestinal conditions, in addition to neratinib and loperamide. A third cohort received addon colestipol, a bile acid sequestrant, in addition to neratinib and loperamide. See Figure 1 for more information on the dosing schedules.
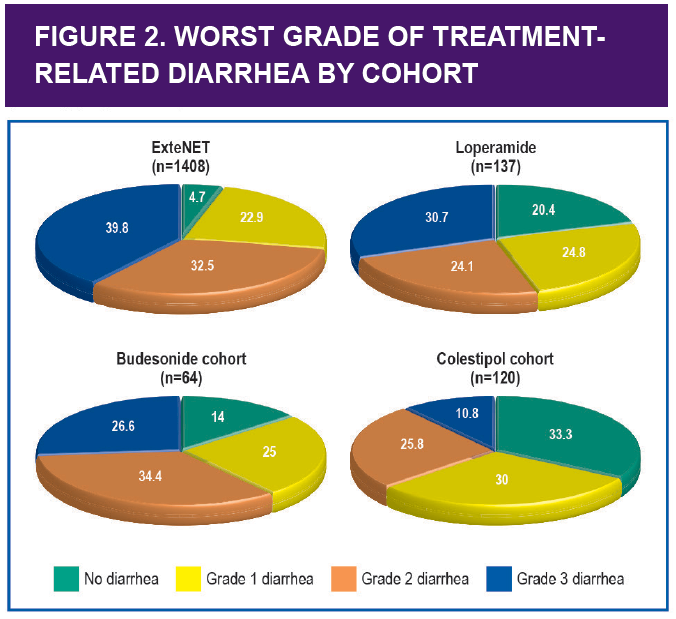
The three cohorts were assessed based on incidence of grade 3 or higher diarrhea (primary endpoint). The results demonstrated that the addition of colestipol to loperamide prophylaxis resulted in the greatest reduction in diarrhea incidence and severity compared with rates observed in the ExteNET trial. See Figure 2 for all outcomes on treatment-related diarrhea from the two trials.
The median cumulative duration of diarrhea and the median number of diarrhea episodes per patient were reduced in those treated with loperamide prophylaxis given with or without budesonide or colestipol compared with the ExteNET control group (http://www.pumabiotechnology.com/docs/040417_Poster_for_CONTROL_Abstract_CT128_AACR17.pdf).
The proportion of patients requiring neratinib dose holds and reductions was also reduced with loperamide prophylaxis when given with or without budesonide or colestipol compared with the ExteNET control group. Treatment discontinuations because of diarrhea in the first cycle (one month) were lower in the budesonide and colestipol cohorts (http://www.pumabiotechnology.com/docs/040417_Poster_for_CONTROL_Abstract_CT128_AACR17.pdf) compared with the loperamide-only cohort.
Effective diarrhea prophylaxis may help to improve the tolerability of neratinib, enhance long-term adherence to treatment, and achieve the best outcomes. A structured loperamide prophylactic regimen for one or two cycles with or without the addition of budesonide or colestipol for a single cycle reduces the incidence, severity, and duration of neratinib-associated diarrhea compared with that seen in the ExteNET trial (http://www.pumabiotechnology.com/docs/040417_Poster_for_CONTROL_Abstract_CT128_AACR17.pdf).
Other Methods for Managing Diarrhea
In addition to prophylaxis, dietary changes may need to be considered, including:
- Stop all lactose-containing products.
- Drink 8–10 large glasses (approximately 2 liters) of clear liquid per day.
- Eat frequent small meals.
- Recommend a low-fat diet enriched with bananas, rice, applesauce, and toast (BRAT diet).

Conversations With Experts
Q: Results of the ExteNET trial indicate that diarrhea is a likely adverse reaction (AR) when patients take Nerlynx® (neratinib) tablets. Diarrhea most often occurs upfront, and taking prophylaxis has been shown to help reduce the incidence and severity. How would you counsel a patient about what to expect before starting treatment?
A: I always make sure patients have information about potential ARs from the very beginning. I explain that 95% of patients in the ExteNET clinical trial experienced some grade of diarrhea with neratinib; however, we will discuss a plan to hopefully prevent, or at least decrease the severity. I talk to patients about the scoring of different grades of diarrhea based on the number of stools per day, and then I go over the prophylaxis regimen, which I strongly encourage them to follow.
Q: How is neratinib-related diarrhea different from that seen with other oncologic agents?
A: With other oncologic agents, diarrhea is often a direct toxicity of chemotherapy; the gastrointestinal epithelium, consisting of rapidly dividing cells, becomes damaged. This results in inflammation and malabsorption, which can then cause diarrhea. Neratinib-related diarrhea is generally time limited, decreasing or resolving as the patient continues on the drug. If we can get through the first two months of treatment, the diarrhea should decrease in severity or, hopefully, resolve entirely. I explain that we can often prevent or significantly limit the diarrhea with a prophylaxis regimen.
Q: How would you advise patients to manage neratinibrelated diarrhea?
A: I think the information that patients get at the very beginning is most important. If they understand the short duration of treatment-related diarrhea, the possibility of dose modifications, and prophylaxis options, they are more apt to get through the treatment.
I ask patients to keep a diary of their bowel movements for our review with each appointment. I encourage them to call if they notice a significant change in their usual schedule, whether that be increasing constipation or increasing number or consistency of their stools. With the diary, we can understand what symptoms they are experiencing and discuss potential solutions to improve quality of life.
Q: When do you advise patients to call the office if they experience diarrhea with neratinib?
A: I encourage close communication. I ask patients to keep track of consistency and frequency of their stools. The diary helps them with this. It involves them more directly in their own care and gives them a sense of empowerment. Our goal is one to two stools per day, and we have patients call us if their schedule varies from our desired plan. If they are having excessively watery stools, which can affect their hydration, we definitely want to intervene before it gets out of control and leads to more potentially significant ARs, such as hypotension.
Q: What is the prophylaxis regimen you use for patients starting neratinib? What considerations factor into this decision?
A: Based on the frequency of diarrhea observed in the initial ExteNET trial, I encourage the use of prophylaxis when starting neratinib. I give patients a copy of the manufacturers’ recommended prophylaxis regimen. Initially, loperamide 4 mg three times per day is recommended for the first two weeks of neratinib treatment. Then we decrease to twice-daily dosing of loperamide and decrease from there as needed. We discuss the results of the CONTROL study, letting patients know that we have additional medications available should we not achieve the desired effect with loperamide alone. Based on their grade of diarrhea, we make decisions whether a neratinib dose modification is necessary.
Q: What should nurses be aware of and focus on when managing patients receiving neratinib?
A: Knowing the potential ARs is important: diarrhea, dehydration, abdominal pain, and low blood pressure. I recommend constant communication with patients, asking if they are eating well or losing weight. I also intermittently review their medication list just to make sure nothing new has been added such as a CYP3A4 inhibitor, which can increase the risk of toxicity if taken with neratinib.
Q: If a patient needs a dose hold or reduction on neratinib, how do you help them decide to continue therapy?
A: Again, I emphasize that this symptom is usually limited to the first month or two. I let them know that we can be aggressive with the loperamide or possibly add in one of the other two drugs from the CONTROL trial. If a dose interruption or reduction is required, sometimes restarting at a lower dose makes patients feel more comfortable because they know they are not receiving the full dose that initially made them sick.
We also go back and look at what they have been through already; sometimes that’s a motivator. If we look at the IV chemotherapy, surgery, radiation, and adjuvant treatment they have already been through, that often puts this in perspective. This is just another symptom that we are trying to work through.
Q: Because we know an AR of loperamide can often be constipation, how do you handle this?
A: I make sure patients are optimizing their fluid intake, because that helps with constipation. We can also hold the loperamide dose while continuing neratinib. I also discuss the signs of a bowel obstruction: if it has been 24–48 hours since a bowel movement, in combination with abdominal pain, then I would rather see the patient.
For women with baseline constipation, the loperamide can be a hard sell. I would rather start them on a day or two of neratinib without prophylaxis, and if they experience diarrhea, we can start loperamide then.
Q: What advice would you give patients regarding dietary changes for the management of diarrhea?
A: I would suggest increasing the fluid intake, avoiding high-fat foods, and trying bland foods, such as the BRAT diet (banana, rice, applesauce, toast). They should also try to avoid lactose-containing foods.