




As Americans reduce tobacco use and treatment and diagnosis advance, lung cancer survivorship rates are improving; however, it still remains the second most common type of cancer. The growing population needs appropriate survivorship care.
Late and Long-Term Effects
Treatment approaches often involve multiple modalities that may increase potential side effects and risks. Surgery may be invasive (e.g., pneumonectomy, lobectomy, wedge resection) or minimally invasive (e.g., video-assisted thorascopic surgery or VATS). Long-term postoperative pain, including postthoracotomy pain syndrome, can greatly affect a patient’s quality of life. Pain management options include nonsteroidal anti-inflammatory agents, opioids, antidepressants, antiepileptics, or localized anesthesia, such as nerve blocks.
Surgeries may also produce functional limitations, including reduced shoulder function and long-term shortness of breath. Oncology nurses must routinely assess for and manage symptoms and involve the interprofessional team as needed (e.g., bronchodilators, pain management, pulmonary rehabilitation, physical therapy).
Chemotherapy options commonly include platinum-based regimens, which can lead to peripheral neuropathy, fatigue, and hearing loss. Patients may be prescribed duloxetine for chemotherapy-induced peripheral neuropathy. After assessing for and ruling out or managing other etiologies for cancer-related fatigue (e.g., sleep-wake disturbances), recommend an increase in physical activity. ONS’s Get Up, Get Moving resources can help guide those conversations.
Radiation is sometimes used for metastatic lesions. Side effects may vary depending on the area of the body irradiated and method of radiation delivery, but fatigue and localized skin changes are the most common. Patients with small cell lung cancer may receive prophylactic cranial irradiation, which is associated with cognitive dysfunction and memory loss.
Non-small cell lung cancer diagnosis and work-up generally includes routine biomarker testing to identify driver variants such as EGFR, ALK, BRAF, and ROS1 and targeted therapies. EGRF inhibitors such as erlotinib and gefitinib can lead to acneiform rash and diarrhea. VEGF agents such as bevacizumab can cause hypertension, bleeding, poor wound healing, fistulas, and perforations. Crizotinib and other drugs targeting ALK can cause gastrointestinal side effects like nausea and vomiting, diarrhea, and constipation. Oncology nurses should identify a full side-effect profile for any targeted agents.
One of the primary treatment options for lung cancer, immunotherapy agents may include checkpoint inhibitors such as pembrolizumab and nivolumab that can induce late or long-term effects in any organ, even after treatment is discontinued. They are typically managed with glucocorticosteroids, but additional therapies are necessary for some patients. Pneumonitis may lead to long-term dyspnea with oxygen requirements.
Ongoing Screening and Prevention
Evaluate patients for psychosocial effects, such as fear of recurrence, anxiety, depression, self-blame, financial difficulties, and role changes. Management strategies include support groups, psychological counseling, behavior therapy, social work, and other resources.
Develop an appropriate surveillance plan with close follow-up, history, physical examination, and radiography to evaluate for local or distant recurrence. Include screening recommendations for second cancers, especially for patients who continue to use or with a history of tobacco use, as well as following general age- and sex-appropriate screening guidelines.
Routinely address risk reduction and lifestyle modification, including weight management, physical activity, healthy diet, and smoking cessation. Coordinate care among the entire team, including oncology, primary care, and other specialties.
Sample Lung Cancer Survivorship Care Plan
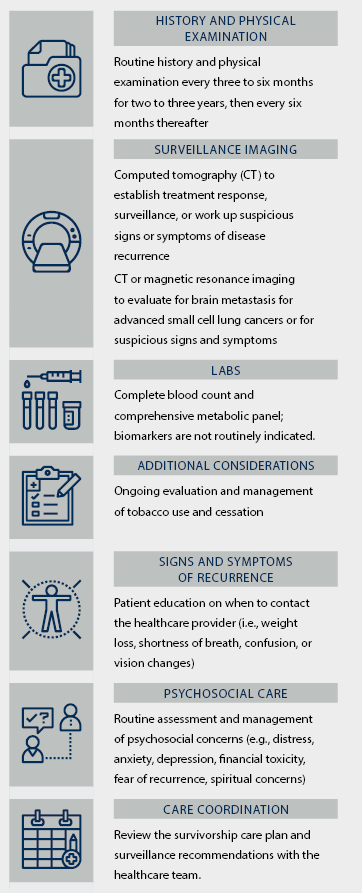
Note. Based on information from NCCN and Vijayvergia et al.