Researchers conducted a randomized study to assess the impact of survivorship care plans (SCPs) on cancer survivors who underwent hematopoietic cell transplantation (HCT).
They assessed confidence in survivorship information (primary analysis), as well as cancer treatment distress, knowledge of transplant exposures, health behaviors, healthcare use, and health general self-efficacy. Navneet S. Majhail, MD, MS, at the Taussig Cancer Institute at the Cleveland Clinic in Ohio, discussed the findings at the ASH Annual Meeting.
Adult survivors were included if they were one to five years post-transplant, proficient in English, and had not relapsed or developed second cancers. Recipients with any diagnosis, HCT and donor type, and conditioning regimen could participate.
The researchers used patient-specific clinical data from the Center for International Blood and Marrow Transplant Research (CIBMTR). They used focus group feedback from patients; caregivers; HCT physicians, nurses, and social workers; and general hematologists/oncologists to design paper-based SCPs. These were developed based on patient risk factors and treatment exposures (e.g., age, sex, HCT type, graft-versus-host disease [GVHD], use of total body irradiation [TBI] or steroids) and published guidelines for long-term follow-up of HCT survivors.
The large, multicenter, randomized study enrolled 495 patients from 17 centers; 458 engaged in a baseline phone survey that included standardized patient-reported outcomes (PROs) related to the study objectives. Patients were then randomized to receive SCP (intervention arm; n = 231) or routine care (n = 227), which was based on their transplant center. The median patient age was 59 years in both cohorts, and most (96% in SCP and 92% in routine care) were white.
Two weeks later, researchers conducted follow-up phone interviews to assess health literacy and ask questions related to the use of SCP for those in the intervention arm. At six months, end-of-study phone PRO surveys were administered; 87% (n = 201) in the SCP group and 88% (n = 199) in the routine care group completed those assessments.
Forty-eight percent of patients in the SCO cohort and 44% in the routine care cohort received allogeneic HCT (alloHCT); 11% and 16%, respectively, had received prior HCT; and 21 and 20%, respectively, had received TBI-based conditioning. Among alloHCT recipients, 63% and 67% had a history of acute GVHD and 60% and 66% had a history of chronic GVHD.
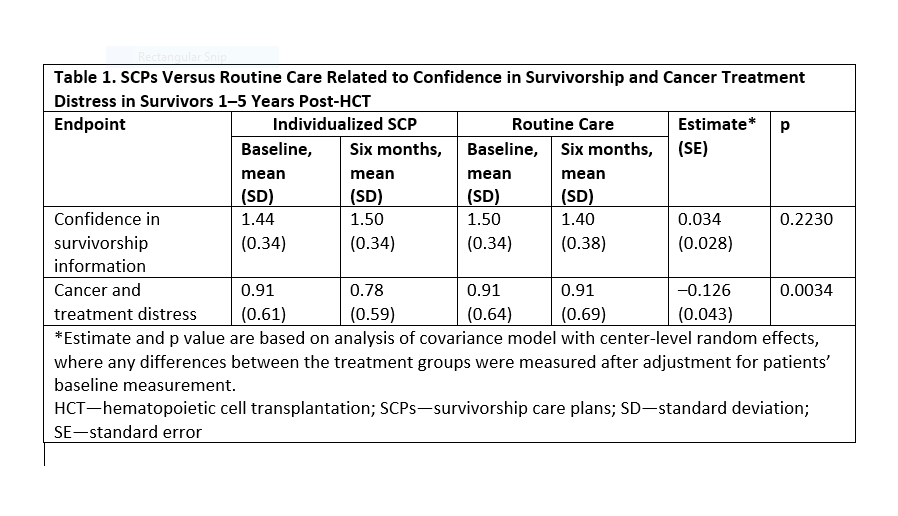
The researchers found that those in the SCP cohort did not see a change in confidence in survivorship information, but cancer treatment distress was significantly reduced (see Table 1). The decrease in cancer treatment distress was independent of sex, transplant type, GVHD status, diagnosis, and health literacy. However, age was significantly associated with cancer treatment distress scores: higher distress was observed among younger patients. However, age had no significant interaction with the SCP effect size. The SCP had no effect on any of the other secondary outcomes.
“We demonstrate that SCPs generated automatically using CIBMTR [individualized] to patient risk-factors, without clinical contact to interpret or personalize the SCP, is feasible and can produce a tool that lowers cancer treatment distress scores at six months in HCT survivors,” the researchers concluded. “Our study supports further development and implementation of individualized SCPs in this population that is at significant risk for late morbidity and mortality from transplantation.”