





By Gean Brown, MSN, RN, OCN®, CNML, and Brianna Lutz, BSN, RN, OCN®

Healthcare institutions have used care delivery models to guide practice for years. A care delivery model provides a structured system for work assignments, responsibilities, and authority to provide optimal patient care.
A team nursing care delivery model enables collaboration with shared responsibility and accountability for all members of the team, which includes the RN and ancillary staff. The patient care delivery model focuses on the RN’s responsibility for the total care of the patient throughout the shift. The primary nursing care delivery model outlines a one-to-one, patient-centered, nurse-patient relationship that promotes continuity of care. The nurse is paired with ancillary staff to assist, but the nurse is ultimately responsible for the patient’s entire length of stay. In the functional care delivery model, the coordination of care rests on the nurse manager or charge nurse and tasks are delegated through a hierarchical structure.

Planning During a Pandemic
Smilow Cancer Hospital, part of Yale-New Haven Health System in Connecticut, was at the forefront of the COVID-19 coronavirus pandemic. Leaders needed to make nimble changes, including reallocating human resources. Many oncology nurses were deployed to new COVID-19 units. As a result, we formed an oncology nursing leadership team to develop a plan to prepare for staff shortages while still providing safe, quality care.
Cancer and COVID-19
Immunocompromised patients with cancer face a higher risk of morbidity and mortality from COVID-19. However, they still need to receive treatment and care during the pandemic. Continuing to deliver high-quality cancer care in the face of a pandemic was a priority; therefore, we developed an emergency staffing plan using the functional care delivery model.
Process
The goal was to determine a safe strategy for reallocating nurses across roles and locations. The first step was compiling a skills inventory to identify tasks that were in and out of scope for nurses and those that required education because staff would be flexing outside of their traditional roles. Nursing leadership completed a staffing level assessment that compared ratios during the usual state to the current COVID-19 state.
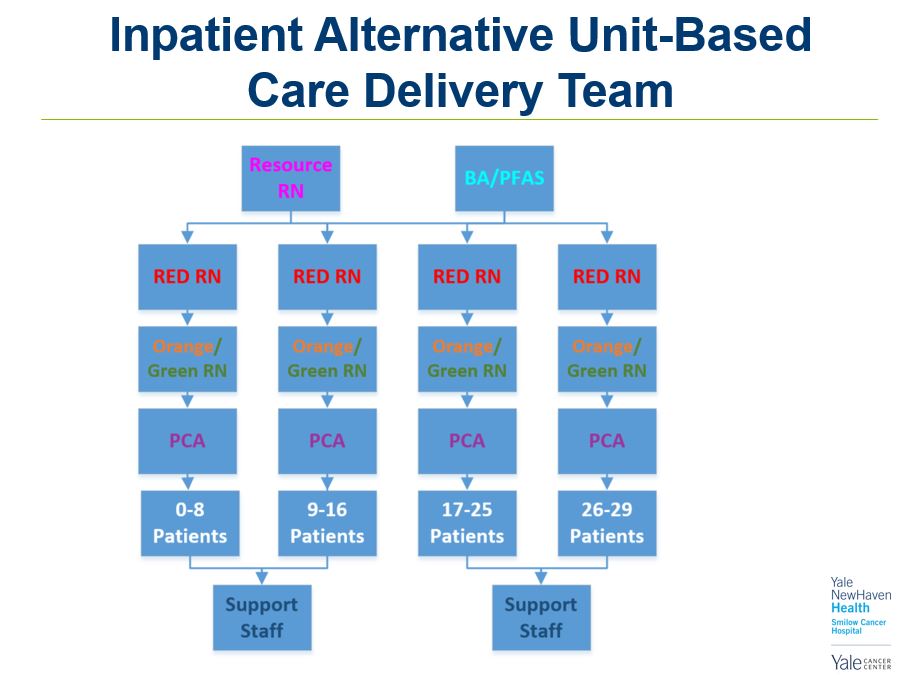
We color coded each nursing role; each team contained one red inpatient oncology nurse, one orange inpatient non-oncology nurse or green ambulatory oncology nurse, and a purple care associate. Each team would care for an eight-patient assignment with the assistance of a resource nurse, unit-based nursing leadership, and ancillary staff.
In the usual state, one red nurse cares for a four-patient assignment, but with the functional model in the pandemic state, the same volume of patients can be safely cared for by half the number of expert primary nurses. Although the number of primary red nurses decreased, the number of total nurses remained the same with support from orange or green nurses. The model allows those with inpatient oncology expertise to stretch nurse-to-patient ratios and cover larger patient zones.
Additional considerations included temporary modifications of functions that do not compromise holistic patient care but do contribute to streamlined nursing care. We also defined the tiers that would trigger the model’s implementation.
The team developed a communication and education plan to support implementation. The education plan includes a nursing skill and competency self-assessment, which the oncology educator uses to determine which nurses are most appropriate for redeployment.
Although we haven’t had to activate the plan yet, we are prepared and ready to meet the needs if we face a second wave or future disasters.