





Because of the risks and dangers associated with hazardous drugs (HDs), guidelines surrounding their use and handling have been issued since 1981. Since then, several organizations, including ONS, the American Society of Health-System Pharmacists, the Occupational Safety and Health Administration, and the National Institute of Occupational Safety and Health (NIOSH), have released guidelines for various providers who handle the drugs.
In 2016, the U.S. Pharmacopeial Convention (USP), which sets standards for quality and purity of medications, published its own standards for safe handling procedures and engineering, known commonly as USP <800>. As a pharmacy-centric organization, much of USP’s standards are focused on pharmacy practices, but several areas of USP 800 relate to the administration of HDs, including directing, monitoring, and enforcing nursing practice.
In his article in the April 2017 issue of the Clinical Journal of Oncology Nursing, Seth Eisenberg, RN, OCN®, BMTCN®, discussed the elements of USP <800> that pertain to oncology nurses and what nurses and institutions need to consider in preparation for implementation and compliance by July 1, 2018. (Editor's note: Since publication of this article, USP has changed the implementation date to December 1, 2019.)
Personal Protective Equipment
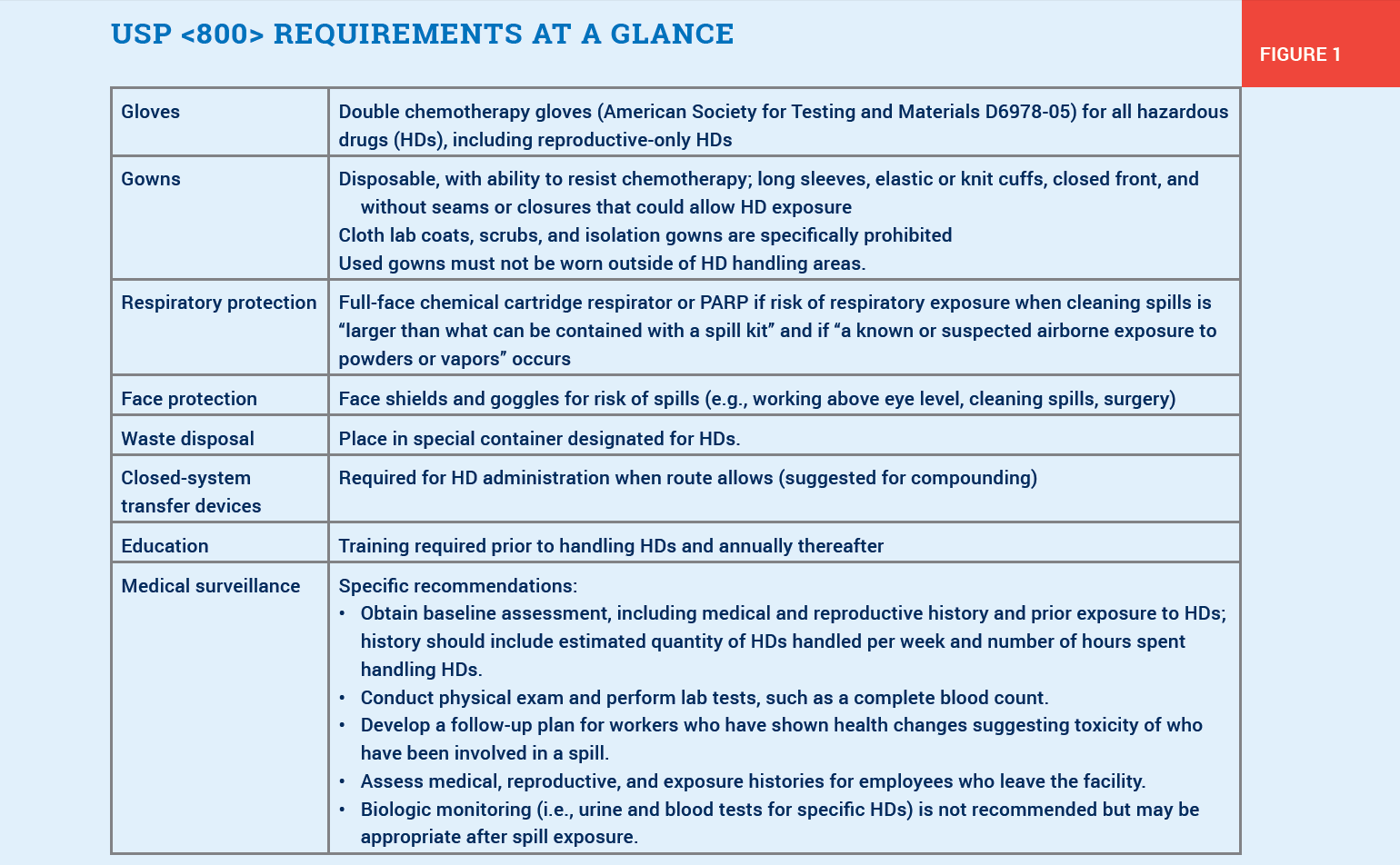
USP <800> requires double gloving for hazardous drug administration, using gloves designated for chemotherapy that conform to the American Society for Testing and Materials D6978-05 standard. It also specifies the use of disposable gowns that are able to resist hazardous drug exposure, and Eisenberg noted that not all gowns have been tested.
Respiratory protection has been a confusing topic in other guidelines, but USP <800> provides some clarification, Eisenberg said. USP <800> does not recommend respiratory protection for administration, but it does require a full-face chemical canister respirator or powered air-purifying respirator (PARP) with a chemical cartridge for dealing with larger spills that cannot be contained in a spill kit or for drugs that can produce vapors at room temperature.
Closed-System Transfer Devices (CTSDs)
CTSDs prohibit the escape of HDs into the environment, and guidelines from ONS and NIOSH recommend their use. USP <800> requires their use for HD administration, which Eisenberg cited as the single most significant change in practice for many nurses, particularly those outside of oncology settings.
Eisenberg described two major CTSD components. The first prevents the release of aerosols, vapors, and droplets during compounding, to protect the pharmacist and technicians and to ensure the exterior of the HD IV bag or syringe is not contaminated. The second protects nurses when transferring the HD from the vial to the IV bag by preventing leaks.
CTSDs can be classified as either a membrane-to-membrane device or a luer-to-luer device, Eisenberg explained. For information on each of the specific available CTSD models, refer to the full article by Eisenberg.
Communication and Education
USP <800> requires organizations “to have an HD program in place that includes policies and procedures delineating how drugs are handled from entry into the facility (e.g., receipt at the pharmacy) through disposal after administration,” Eisenberg explained. Facilities must also document handing precautions for oral agents separately from other dosage forms.
RNs must be educated on safe HD practices before working with the drugs. Annual competency assessments and documentation are required. Key components of an HD plan, including education, are:
- An overview of the written plan that describes how the HD standard will be implemented
- Annual assessment of risks associated with HD handling
- Annual listing of all HDs administered in the facility
- HD-specific safety education, including review of policies and procedures, before new staff can handle HDs
- Annual subsequent training on the proper use of personal protective equipment and CTSDs
- Easy access to safety data sheets for HDs administered in the facility
- Written confirmation by all staff with reproductive capability that the risks are fully understood.
Surveillance
USP <800> recommends that personnel who handle HDs should be part of a medical surveillance program. Eisenberg noted that although it is not required, USP <800> reinforces the recommendations included in NIOSH’s guidelines:
- Obtain baseline physical assessment and medical history on all personnel involved with HD handling, including
- Reproductive history and prior exposure to HDs
- Estimated quantity of HDs handled per week
- Number of hours spent handling HDs
- Lab testing (e.g., complete blood count).
- Monitor prospective changes in health, particularly after a known exposure (i.e., spill).
- Provide follow-up for employees who develop symptoms that may be related to exposure.
- Individuals displaying health changes related to exposure should prompt an immediate evaluation of all of the organization’s preventive safeguards.
- Perform a reassessment exam when an employee departs the organization.
For more information on USP <800> and the implications for oncology nurses, refer to Eisenberg’s full article.
This monthly feature offers readers a concise recap of full-length articles published in the Clinical Journal of Oncology Nursing (CJON) or Oncology Nursing Forum. This edition summarizes “Hazardous Drugs and USP <800>: Implications for Nurses,” by Seth Eisenberg, RN, OCN®, BMTCN®, which was published in the April 2017 issue of CJON. Questions regarding the information presented in this article should be directed to the CJON editor at CJONEditor@ons.org. Photocopying of this article for educational purposes and group discussion is permitted.