




Immunotherapy has evolved into the “fourth pillar” of cancer care, along with surgery, chemotherapy and radiation therapy, according to Laura S. Wood RN, MSN, OCN®, of the Cleveland Clinic Taussig Cancer Center in Ohio and Krista M. Rubin, MS, RN, FNP-BC, of Massachusetts General Hospital in Boston, who spoke during a session on Wednesday, April 10, 2019, at the ONS 44th Annual Congress in Anaheim, CA. Immunotherapeutic agents, however, are vastly different from chemotherapies and have a distinct toxicity profile that advanced practice nurses must be familiar with.
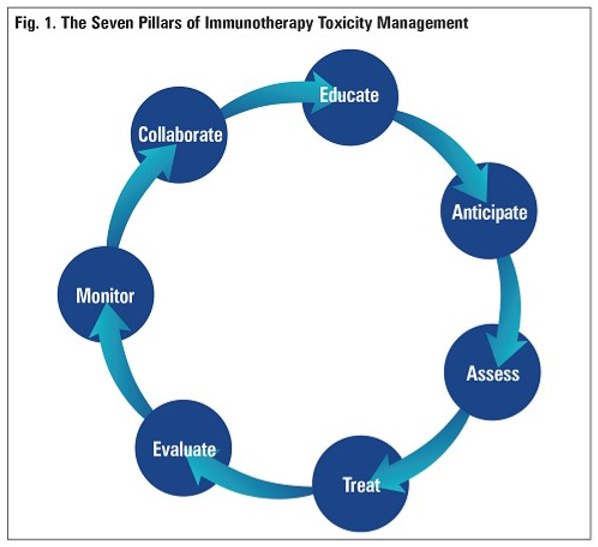
Immune-related adverse events (irAEs) are diverse, potentially affecting almost any body system. The successful management of irAEs has seven key components (see sidebar).
Tools to Manage irAEs
Several professional organizations involved in caring for patients receiving immunotherapy, including the American Society of Clinical Oncology (ASCO) and the Society for Immunotherapy of Cancer (SITC), have developed guidelines for managing irAEs. Most of the guidelines are algorithm based and offer management recommendations based on the Common Toxicity Criteria for Adverse Events grading system.
Key points in the ASCO guidelines include:
- Provide patients and caregivers with timely, up-to-date education about immunotherapies, including their mechanism of action and the clinical profile of possible irAEs.
- Maintain a high level of suspicion that new symptoms are treatment related.
- Grade 1 irAEs: Except in the case of some neurologic, hematologic or cardiac toxicities, continue therapy with close monitoring and provide supportive care.
- Grade 2 irAEs. Hold therapy, treat with low-dose prednisone or equivalent, and increase the dose in 2 to 3 days if no improvement is seen.
- Grade 3 irAEs: Hold therapy, treat with high-dose prednisone or intravenous methylprednisolone, and slowly taper the steroid over 4 to 6 weeks. Consider additional interventions if no improvement is seen in 48 to 82 hours.
- Grade 4 irAEs: Permanently discontinue immunotherapy, except in endocrinopathies that have been controlled with hormone replacement therapy.
- Consider resuming therapy when symptoms and laboratory values improve to Grade 1.
According to the SITC guidelines, detailed pretreatment screening is important, including history, blood tests (e.g., HgbA1c, total CK, fasting lipid profile). Patients with pre-existing organ disease should also be screened for cortisol and adrenocorticotropin as well as brain natriuretic peptide (BNP) or N pro-BNP and should undergo pulmonary function tests.
The SITC guidelines focus on the clinical presentation and epidemiology of each irAE and encourage referral and multidisciplinary care. Specific recommendations include:
- Grade 2 irAEs: Start low-dose oral prednisone if indicated, hold immunotherapy during steroid use, and start a proton pump inhibitor for gastrointestinal irAE prophylaxis.
- Grade 3 irAEs: Start high-dose prednisone or methylprednisolone and add Pneumocystis carinii pneumonia prophylaxis if more than three weeks of immunosuppression are expected.
- Grade 4 irAEs: Start high-dose prednisone. If no improvement is seen in two to three days, add an additional immune suppressant (e.g., infliximab). Discontinue immunotherapy.
More information and tools for irAE management are readily available online, including ONS’s immunotherapy wallet cards and other immunotherapy resources.